HIPAA-aligned LLM deployment is the practice of running large language models inside a healthcare environment such that protected health information (PHI) never leaves the covered entity’s control. It requires a signed Business Associate Agreement, privacy-preserving data flow, role-based access controls, encryption in transit and at rest, immutable audit logs, and contractual guarantees against training-data leakage. Most public LLM APIs do not meet this bar by default — and the AIVeda private AI for healthcare practice was built specifically to close that gap.
| Healthcare buyers should treat HIPAA as an architectural constraint, not a checkbox at the end of a procurement cycle. |
Why generic LLM APIs fail HIPAA out of the box
HIPAA governs the use, storage, and disclosure of PHI under the Privacy Rule, Security Rule, and Breach Notification Rule. The U.S. Department of Health and Human Services Office for Civil Rights has issued more than $137 million in HIPAA settlements since 2016, and cloud or AI misconfigurations now account for a rising share of the caseload.
Public consumer endpoints — ChatGPT, generic Claude, Gemini consumer tiers — typically violate one or more HIPAA requirements out of the box.
- Standard terms of service do not include a signed Business Associate Agreement.
- Inputs may be retained for model training or telemetry without granular customer control.
- Audit logging is consumer-grade and rarely meets HIPAA’s six-year documentation standard.
- Geographic data residency is fixed by the provider, not the customer.
- No contractual mechanism exists for breach notification inside the required 60-day window.
Even where an enterprise BAA is available — OpenAI offers one at the enterprise tier and Anthropic does the same for qualifying customers — questions remain about subprocessor flows, fine-tuning data lineage, and inference logging. A signed BAA is a starting point. It is not a finish line. For a deeper teardown, see our companion guide on HIPAA-compliant private LLM deployment patterns.
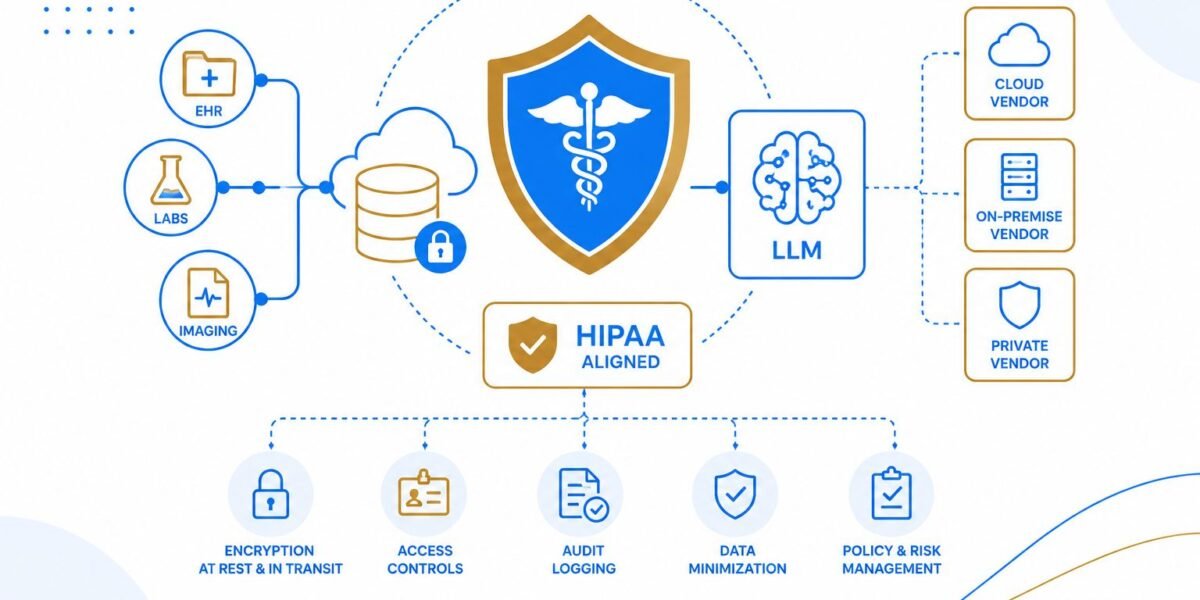
Reference architecture: the six structural components
A defensible HIPAA-aligned LLM deployment is built from six independent control layers. Each one is a HIPAA boundary in its own right; removing any single layer is sufficient to put a covered entity out of compliance. The pattern below mirrors what we deploy under the AIVeda Private LLM Development service.
1. Private model hosting
The model — whether Llama 3, Mistral, MedLM, Med-Gemini, or a fine-tuned open-weights variant — runs inside the covered entity’s on-premise data centre, a customer-controlled VPC, or a HITRUST-certified private cloud. No PHI crosses the boundary into a multi-tenant model provider. This is the single highest-leverage architectural decision and the foundation of every AIVeda enterprise deployment model. For a hardware-and-sizing walkthrough, see our on-prem LLM deployment guide.
2. PHI-safe data layer
A vector database — Pinecone, Weaviate, Qdrant, or pgvector — holding embeddings of clinical documents must itself live inside the controlled environment, encrypted with customer-managed keys, with access scoped per service account. Embedding leakage is the most underestimated vector for unintentional PHI disclosure: under known-plaintext conditions, sentence embeddings can be partially reversed (Pan et al., 2020, IEEE S&P). The AIVeda Secure RAG framework addresses this with citation-bound retrieval and per-tenant key isolation.
3. De-identification gateway
Before any text reaches the model, a deterministic redaction layer strips the 18-category Safe Harbor identifiers using regex plus a clinical named-entity-recognition model. For high-risk corpora — oncology, behavioural health, rare disease — the Expert Determination method applied by a qualified statistician is the preferred standard, since quasi-identifiers (rare diagnoses, employer names, dates of admission) can re-identify patients with as few as three data points (Sweeney, 2000, Carnegie Mellon).
4. Role-based access control
Every query is authenticated against the covered entity’s identity provider — Okta, Azure AD, or on-prem Active Directory — and scoped to a clinical role: attending physician, resident, nurse, billing analyst, research coordinator. The model only sees the data the user is contractually authorised to see. RBAC sits inside our broader AI Governance and Compliance practice.
5. Immutable audit logging
Every prompt, response, retrieved chunk, and access decision is written to an append-only log (Splunk, Datadog, CloudWatch Logs Insights) with the six-year retention HIPAA requires for documentation. The audit logs themselves are PHI under the rule and must be encrypted and access-controlled.
6. Encryption in transit and at rest
TLS 1.3 for transport. AES-256 at rest. Customer-managed keys via AWS KMS, Azure Key Vault, or HashiCorp Vault — never keys held by the model provider. Bring-your-own-key (BYOK) is the minimum bar for any healthcare deployment in 2026. NIST SP 800-66 Revision 2 provides the authoritative implementation guidance.
Vendor selection: six dimensions that matter
Healthcare CIOs evaluating LLM vendors should score each candidate across the six dimensions below. A score of zero on any dimension is a hard disqualification.
Deployment model
Does the vendor support on-premise, customer-VPC, or HITRUST-certified private cloud deployment? If the only option is a multi-tenant API endpoint, the vendor is out for any workflow that touches PHI. Compare against the three deployment patterns AIVeda supports — on-prem, VPC private AI, and hybrid.
Business Associate Agreement
Will the vendor sign a HIPAA BAA covering inference, fine-tuning, telemetry, and downstream subprocessors? Review the BAA carefully for carve-outs around aggregated metrics and product analytics — vendors sometimes exempt these even though they can constitute PHI under HIPAA’s minimum-necessary standard. HHS publishes sample BAA provisions that buyers can use as a baseline.
Model ownership and inference isolation
Is the model dedicated to the customer, or shared across tenants? Is there any path through which one customer’s queries could influence another customer’s responses? Multi-tenant fine-tuning is a red flag and rarely disclosed in vendor sales materials. The AIVeda Private LLM Engineering team walks customers through dedicated-model architectures end-to-end.
Compliance certifications
HITRUST CSF certification is the de facto industry standard for healthcare cloud workloads. SOC 2 Type II is necessary but not sufficient. Buyers handling clinical decision support should also confirm FDA 21 CFR Part 11 alignment, and the NIST AI Risk Management Framework provides the controls library for everything above and beyond HIPAA.
Observability and audit
Can administrators inspect every model call, every retrieved chunk, every access decision? Can the audit feed be streamed to the customer’s SIEM? Black-box endpoints fail this test. The observability stack we ship as part of Secure AI Deployment and MLOps covers prompt, retrieval, decision, and outcome telemetry by default.
Cost predictability
Token-based pricing is unpredictable at clinical scale. A 200-bed hospital running ambient scribing across 600 daily encounters can burn $35,000–$45,000 per month on a public API at current rates. Private deployment converts the cost structure to a fixed infrastructure line, typically 60–70% lower per encounter at production scale — small language models bring the unit economics down further for narrow workflows.
Quick comparison: deployment options
| Dimension | Public LLM API | Enterprise Private LLM | Custom Private LLM |
| HIPAA BAA | Limited tiers | Yes | Yes |
| Data residency | Provider-chosen | Customer VPC | On-prem / VPC |
| Model isolation | Multi-tenant | Dedicated | Dedicated + owned |
| Audit logging | Consumer-grade | Enterprise | Full custom |
| Fine-tuning rights | Restricted | Allowed | Full ownership |
| Cost at scale | Unpredictable | Predictable | Lowest per token |
Three pitfalls that trap healthcare buyers
Pitfall 1 — Treating the BAA as a compliance shield
A BAA is a legal contract that assigns liability. It does not prevent breaches and it does not substitute for technical controls. Buyers who assume “we have a BAA, so we are compliant” are the ones who appear in OCR settlement reports.
Pitfall 2 — One-time de-identification
Real clinical text contains quasi-identifiers that re-identify patients even after the 18 Safe Harbor identifiers are stripped. Continuous risk monitoring and Expert Determination by a qualified statistician are required for sensitive specialties — see the Sweeney CMU study on demographic identifiability for the foundational evidence.
Pitfall 3 — Treating the LLM as the only attack surface
The vector database, the retrieval pipeline, the prompt cache, and the audit log are all PHI repositories under HIPAA. Each needs its own access controls, encryption, and retention policy. Securing only the model leaves five doors open. The AIVeda Secure RAG reference architecture addresses every one of those surfaces.
Frequently asked questions
Is HIPAA compliance possible with public LLM APIs?
Only when the vendor offers a signed BAA, contractual guarantees on training-data use, full audit logging, and a clear breach-notification mechanism. Most consumer-grade endpoints do not qualify; some enterprise tiers do, with significant configuration.
Do open-source models like Llama or Mistral make a system HIPAA-compliant?
The model itself is not a HIPAA control. What matters is where it runs, who can access it, how data flows in and out, and whether the surrounding architecture meets the Security Rule. Open weights enable private hosting; they do not enforce it.
What is the difference between de-identification and anonymisation?
HIPAA recognises two standards: Safe Harbor (remove 18 specified identifiers) and Expert Determination (statistical confirmation that re-identification risk is very small). Anonymisation is a stricter, often irreversible standard typically used in GDPR contexts.
How long does a HIPAA-aligned LLM deployment take?
A pilot covering one workflow — ambient scribing, prior authorisation, claims summarisation — can move from contract to first production user in 60–90 days. Enterprise rollout typically follows in 6–9 months.
What is the role of HITRUST CSF certification?
HITRUST is the de facto industry standard for healthcare cloud and AI workloads. It combines HIPAA, NIST 800-53, ISO 27001, and PCI DSS into a single certifiable framework, and it materially reduces audit overhead for the covered entity.
Bottom line
Deploying LLMs in healthcare is not a model problem. It is an architecture problem. The covered entities that move from pilot to production fastest are those that treat HIPAA controls as foundational design constraints, not bolt-on compliance. If you’re evaluating where to start, our Private AI Strategy and Advisory practice runs a structured readiness assessment that maps your existing workflows against the architecture above.
| AIVeda builds and operates HIPAA-aligned LLM deployments for hospitals, payers, and clinical SaaS companies — private hosting, BAA-backed, HITRUST-aligned, audit-ready. |
To explore an architecture review for your environment, contact hello@aiveda.io or book a Private AI Readiness Audit.